
















")










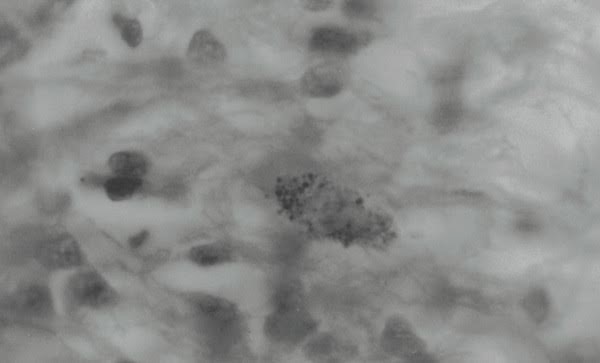 Tissue section of Hodgkin’s disease (lymphoma) of the lung showing a cell with intracellular
granules and coccoid forms (microzymas?) Gram stain, x1000, in oil.
Tissue section of Hodgkin’s disease (lymphoma) of the lung showing a cell with intracellular
granules and coccoid forms (microzymas?) Gram stain, x1000, in oil.
by Alan Cantwell, M.D. Copyright 2017
Editor’s note: Part I was about the origin of life and the Béchamp-Pasteur clash: In the attempt to “classify” laboratory-grown bacteria as the lowest forms of life known in the late nineteenth century, there was no consideration given to any possible “connection” between any of the various species of bacteria.
The dogma was that a coccus remained a coccus; a rod remained a rod; and there was no interplay between them. There was also no “crossing over” from one species to another, and the research by the pleomorphists which suggested otherwise was ignored.
When viruses were discovered they were made separate from bacteria, although bacteria are also known to be susceptible to viral infection.
Viruses were put in one box; bacteria in another. As a result, the spectacular number of “filterable” pleomorphic microbial forms that form a bridge between the “living” bacteria and the “dead” viruses are still largely unstudied and considered of no great importance in clinical medicine.
Thanks to Pasteur, common “skin” bacteria like cocci and bacilli are often viewed as suspicious laboratory “contaminants” or “secondary invaders” or “opportunistic infections” of no great importance as etiologic agents.
As a result of all this dogma and rigidity, medical thought was completely turned off to the possibility that certain cancers and chronic diseases might be caused by common pleomorphic bacteria originating in our own body cells.
Antoine Béchamp’s idea that bacteria could arise from damaged human cells was deemed preposterous.
The legacy of Béchamp
Béchamp described the earliest stages of cellular microzymas as “granules.” Using a light microscope at its highest power, at a magnification of 1000 times.
I don’t think it’s yet possible to definitively point to a single “granule” and claim it is a microzyma. A study of human microscopic pathology reveals the presence of countless granules in blood and tissue.
However, because suitably-stained bacteria are visible at this magnification they are able to be identified. The appearance of blood and tissue bacteria associated with cancer and certain chronic diseases has been described by various (and always controversial) researchers.
This research goes back to the dawn of microbiology in the late 1890s, when doctors finally accepted germs as a cause of disease. Unfortunately, modern doctors still do not accept bacteria that have been studied and reported in cancerous tissue and claimed to be the cause of cancer. Some vehemently oppose such a belief.
There are numerous scientists who owe a debt to Béchamp and his contention that human disease has its roots within the cells of the body itself. Cells are damaged. The microzymas within the cell react to this damage.
Microbes develop from microzymas within the damaged cells, resulting in cellular inflammation and disease production.
In 1890, William Russell, a renowned Scottish pathologist, described “the parasite of cancer” that he discovered in every cancer he examined.
German zoologist Gunter Enderlein (1872-1968) studied aspects of the microbes emanating from microzymas, labelling them as “protits” and described a “life cycle” for these pleomorphic organisms.
Canadian microbiologist Gaston Naessens (born 1924) has also studied the life cycles of blood microbes, which he defines as “somatids” and other forms.
With his specially-designed microscope capable of time-lapse microphotography, Royal Raymond Rife (1888-1971) was the first to directly visualize viruses and transformations of pleomorphic bacteria in human tissue. Rife’s scientific achievements are recounted by Jeff Rense on Rense.com.
Undoubtedly related to Béchamp is the cancer research of the highly controversial Wilhelm Reich (1897-1957), whose studies and conclusions concerning “bions” and “T-bacilli” derived from cancerous cells eventually landed him in an American prison where he died.
My mentor, Virginia Livingston (1906-1990), along with her co-workers, spent a lifetime in research preaching that cancer was caused by pleomorphic acid-fast bacteria. For more on these two physicians, see ‘Virginia Livingston: Cancer quack or medical genius?’ and ‘Dr. Wilhelm Reich: Scientific genius—or medical madman?’ on Rense.com
Despite the general belief that normal, healthy human blood is “sterile,” there is more and more evidence that human blood harbors bacteria normally, both in health and disease.
These bacteria have been determined to be staphylococcal, streptococcal, and corynebacteria-like pleomorphic cell wall deficient bacteria, some of which are acid-fast. For examples of direct viewing of microscopic findings of bacteria in normal blood, please see Tom Detwiler’s website (www.bloodmicrobe.org).
Microzymas, tissue granules and coccoids, and cell wall deficient bacteria
How are microzymas related to the bacterial theory of cancer? According to Virginia Livingston and others, the cancer germ is an intra- and extracellular bacterium that can be identified by special staining of cancerous tissue, particularly the acid-fast stain—a stain traditionally used to detect TB bacteria.
Cancer bacteria are pleomorphic, some of the largest “large body forms” even attaining the size of red blood cells. The most common form in tissue is the granular (coccoid) form.
However, pathologists do not accept the idea that these tissue bodies are microbial in nature. The larger bodies are sometimes interpreted as “Russell bodies” of dubious origin, but never as Russell’s “parasite of cancer.” (For more on large bodies, see my online article: ‘The return of the cancer parasite.’)
If bacteria evolve from the microzymas within the cell, as Béchamp proposed, the first appearance would be the formation of granules and coccoid forms intracellularly.
The micro-photographs below show examples of how these granules (microbial coccoid forms) might appear in cancerous tissue, such as in AIDS-related Kaposi’s sarcoma of the skin, breast cancer, and prostate cancer. See above photo for Hodgkin’s disease (lymphoma).
Béchamp and the future of medical science
At the turn of the 21st century a remarkable acknowledgment took place. Scientists now believe that that the majority of our body cells are not human cells. On the contrary, 50% of our cells or more are estimated to be microbial cells, mostly bacteria. There are over 37 trillion cells in our bodies.
What role do our trillions of body microbes play in the chronic diseases of aging and in cancer? At present, we don’t know. We now recognize these germs are scattered in various tissues and organs of the body once thought to be sterile. And the blood contains bacteria that undoubtedly are carried to every cell in the body.
I have long been asking Why do doctors object so strongly when a scientist concludes that bacteria (rather than viruses) play a role in cancer? And are doctors failing to recognize bacteria in cancerous tissue?
Whatever the answer, the role of bacteria in cancer will have to be settled once and for all. In the meantime, we continue to ignore cancer microbe research to the detriment of the patient.
Pasteur was the genius of his day; and Béchamp’s microzymian theory and contrary views were an annoyance to the Academy.
The medical establishment knew how to deal with rebels like Antoine Béchamp (1816-1906). His work would be ignored by the “authorities” and never cited by the “experts.” His ideas would never be taken seriously in journals and textbooks.
Biomedical editors would purge his name from the pages of their scientific publications. Béchamp would quickly vanish from the annals of science. This is the way all medical rebels are silenced by the establishment.
Suggested reading: (These articles can be found on www. Rense.com by using that website’s search engine)
Broxmeyer L and Cantwell A: AIDS: “It’s the bacteria, stupid!” (2008)
Cantwell A: Cancer is an infection caused by tuberculosis-type bacteria. (2008)
Cantwell A: All human blood is infected with bacteria. (2007)
Cantwell A: Do TB-type bacteria cause AIDS? (2007)
Cantwell A: Immortal HeLa cells and the continuing contamination of cancer and vaccine research. (2010)
Cantwell A: The ‘Star Cell’; The microscopic indicator of bacterial infection in cancer, AIDS and chronic disease. (2011)
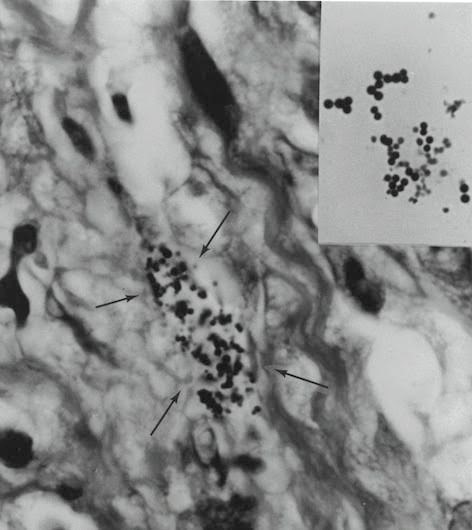
Fite (acid-fast) stained tissue section of AIDS-related Kaposi’s sarcoma of the skin. Arrows point to a collection of variably-sized coccoid forms and granules (microzymas?) in the dermis portion of the skin. Insert shows
Gram-stained Staphylococcus epidermis cultured from the tumor. Note the size and shape of the staphylococci in lab culture which appear similar to those coccoid forms seen in the tumor. Magnification x1000, in oil.
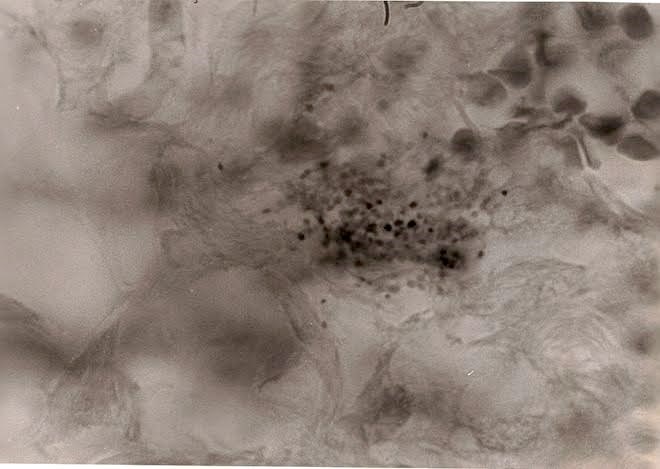 Tissue section of breast cancer showing a group of variably-stained extracellular coccoid forms. Compare the size of these “granules” with the size of a group of red blood cells seen in the upper right. Fite stain, x1000, in oil.
Tissue section of breast cancer showing a group of variably-stained extracellular coccoid forms. Compare the size of these “granules” with the size of a group of red blood cells seen in the upper right. Fite stain, x1000, in oil.
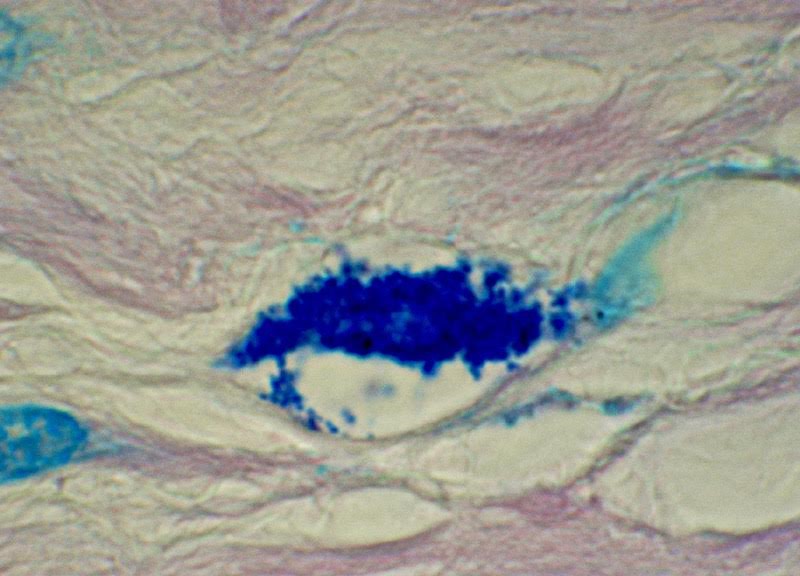 Tissue section of prostate cancer showing a cell laden with intracellular coccoid forms. A few of the forms emanate from the cell and become extracellular. Fite stain, x1000, in oil.
Tissue section of prostate cancer showing a cell laden with intracellular coccoid forms. A few of the forms emanate from the cell and become extracellular. Fite stain, x1000, in oil.
— Alan Cantwell, M.D. is a retired dermatologist and cancer researcher. He is the author of The Cancer Microbe and Four Women Against Cancer, both available from Amazon.com
Re Part 1, I liked Bechamp’s explanation of shed-blood performing its trick of coagulation. So that business casts doubt (to me, a layman) on the explanation of putrefation. Allow me to quote the Wikipedia article on putrefaction with my comments in brackets:
“The breakdown of the proteins of a decomposing body is a spontaneous process. Protein hydrolysis is accelerated as the anaerobic bacteria of the digestive tract [why only of the digestive tract? Even standard medical science today agrees that we are loaded with bacteria] consume, digest, and excrete the cellular proteins of the body.
“The bacterial digestion of the cellular proteins weakens the tissues of the body. As the proteins are continuously broken down to smaller components, the bacteria excrete gases and organic compounds, which carry the noxious odor of rotten flesh. [Oh yeah? Hasn’t anyone – how about the military – experimented to see if some little pleomorphs could be hard at work here? For one thing they need to get out. Don’t they have a life urge like that of their now-defunct host?]
“In the course of putrefaction, the skin tissues of the body eventually rupture and release the bacterial gas. [What did I say?] As the anaerobic bacteria continue consuming, digesting, and excreting the tissue proteins, the body’s decomposition progresses to the stage of skeletonization.”
If any of you farmers reading Gumshoe can help by comparing this to the turn-over of the soil by microbes, please do.
Ashes to ashes, etc.