

















")








by Mary W Maxwell
I am not a physician. I have absolutely nothing to offer in personal research about the delayed effects of cancer treatments. The article at hand is only a regurgitation of James Armitage’s 2010 article, published in the New England Journal of Medicine (NEJM), plus a bit of commentary as to the “sequelae” of his publication.
My general theme is: even when it is noted that a treatment may have harmful effects, the medical industry does not publicize that fact.
Recently, a friend asked me to recall what I had said about “delayed effects” in my 2013 book, Consider the Lilies: A Review of 18 Cures for Cancer and Their Legal Status. I recalled that I had included a one-page bunch of excerpts from Armitage’s article. I shall now print that page here. It was never intended as a final word on the subject. Rather I was making the point, in the concluding chapter of my book, that even when some amazing statistics are presented, they do not necessarily lead to re-thinking about a treatment.
Let me be extra-cautious by pointing out that Dr Armitage was not holding forth about the risks to patients who have radiation treatment for any-and-all types of cancer. As expressed in the title of his article “Early Stage Hodgkin’s Lymphoma,” that disease was his research animal.
My 2013 Page of Excerpts
I wrote the following, having read Armitage’s 2010 article (which anyone can fetch here at the PUBMED website). Any bolding is mine; the original article has none. Please note that there are two separate issues here: the patient’s development later of a second, new cancer (“a second malignant condition,” not to be confused with metastases of the original one), and other illnesses – but here please be aware that Armitage only looked at cardiovascular illnesses.
I believe he was looking only at patients who received BOTH radiation and chemo, as was normal at the time.
Some of the most serious toxic effects of treatment tend to occur late. … the risk of treatment failure is calculated with the use of the International Prognostic Score … defined in selected clinical trials. The frequency of late complications is dependent on the particular treatment used.
The late treatment-related complications of radio-therapy have been studied extensively. … there is an increased incidence of several potentially lethal events after radiotherapy.
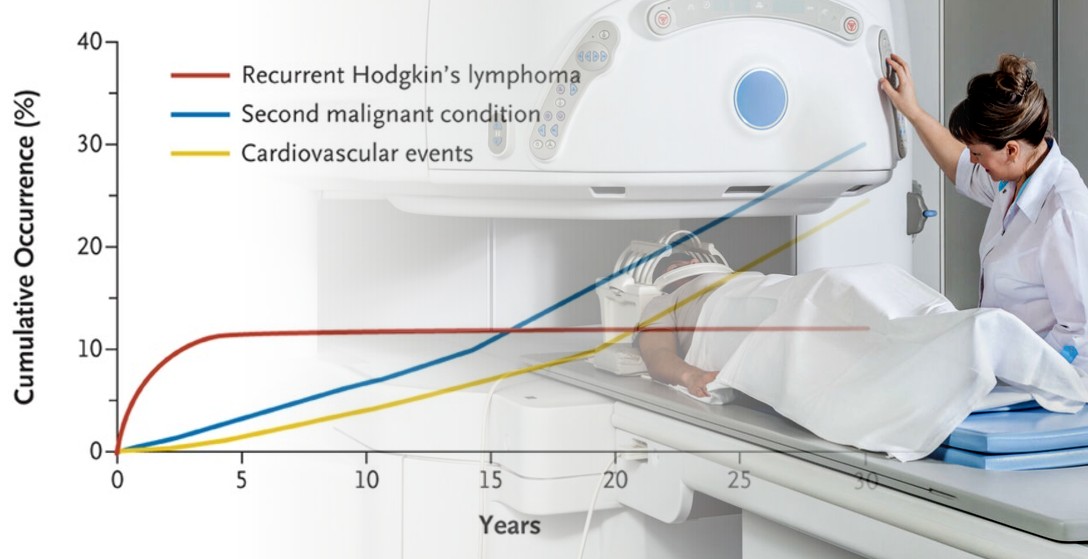
Second malignant conditions occur at an average rate of approximately 1% per year for at least 30 years after treatment. The risk is particularly high among women younger than 30 years of age who receive thoracic radiotherapy; breast cancer develops in 30 to 40% of these patients in the 25 years after treatment. Radiation-related cardiac disease can be manifested as coronary artery disease, myocardial injury, valvular disease, or pericardial fibrosis.
The risk of death from myocardial infarction is increased after thoracic radiotherapy, and that increased risk persists for more than 25 years. Diastolic dysfunction after radiotherapy seems to be a marker for an increased risk of cardiac events. The incidence of stroke also rises in patients who receive radiotherapy in the neck and mediastinum.
Chemo
The risk of late complications after chemotherapy appears to be dependent on the type of drugs prescribed. For example, patients prescribed regimens that include mechlorethamine have a significantly increased risk of myelodysplasia, acute myeloid leukemia, and lung cancer. … Bleomycin, which is also included in the ABVD regimen, is associated with pulmonary fibrosis. The acute pulmonary injury associated with bleomycin can be fatal ….
Consequence of Armitage’s Report
I added, at the bottom of the page (which is p 236 in my Consider the Lilies book): “Who knew? And when did they know it?”
I am not sure how much was known of these problems, prior to 2010 – probably a lot. But in order to help my friend, I have just done a light search of responses to Armitage. There are no comments made to his article in the NEJM (as these would be reported on PUBMED which is blank).
I did find the following article at Medscape Medical News/Oncology by Roxanne Nelson. It doesn’t mention any new directives that have gone out to doctors as a result of Armitage’s report, but hers was printed in 2011, much too soon to reflect such a thing. (Doctors do get directives, all the time.) I also point out that her article focuses only on a comparison between combining chemo and radiation or just having chemo:
Advantage to Radiation Plus Chemo in Hodgkin’s Lymphoma, by Roxanne Nelson
Dr. Armitage, who is from the University of Nebraska Medical Center in Omaha, explains that the risk is particularly high among women younger than 30 years of age who receive thoracic therapy. “Breast cancer develops in 30% to 40% of these patients in the 25 years after treatment,” he writes.
In the new meta-analysis, Dr. Engert and colleagues demonstrate that the addition of radiotherapy to commonly used chemotherapy regimens increased 5-year overall survival and tumor control in patients with early-stage Hodgkin’s lymphoma.
However, this is still an “unsettled treatment issue that goes back 40 years or more,” said Richard Little, MD, a senior oncologist at the National Cancer Institute. “It comes down to the question of late-term side effects associated with radiation,” which is an area that the meta-analysis did not address, he pointed out in a statement released by the Health Behavior News Service.
The follow-up period ranged from 2.0 to 11.4 years, and in all 5 studies, patients who received radiation therapy were no more likely to experience adverse events than those who received chemotherapy alone. Most adverse events were similar in both patient groups and were typical of those seen with chemotherapy. [How interesting.]
The authors do note that long-term effects, such as secondary malignancies or cardiac disease, can occur after the reported observation times of trials. [Emphasis added]
Aritcles in the Guardian and the Independent, on Related Matters
The popular press sometimes alerts us to studies. First I will quote a 2015 article in the Guardian, specifically about an after-effect (loss of cognitive ability) associated with whole-brain radiation, and also about the fate of lymph nodes. Then I’ll quote from The Independent about the fact that new anti-cancer drugs can come onto the market before their effects, or even their treatment-value, is studied.
Treating whole brain with radiation found to harm cognitive skills without improving survival, study finds – meaning many could be spared such care”
The Guardian, from AP: Mon 1 Jun 2015 04.16 AEST; Last modified on Thu 21 Sep 2017
“A major study could change care for many of the hundreds of thousands of people each year who have cancer that spreads to the brain from other sites, study leaders said on Sunday.
The study, one of three discussed at an American Society of Clinical Oncology conference in Chicago, found that contrary to conventional wisdom, radiation therapy to the whole brain did not improve survival, and harmed memory, speech and thinking skills.
‘This is the classic question: Which is worse, the disease or the treatment?’ said one study leader, Dr Jan Buckner of the Mayo Clinic in Rochester, Minnesota. Radiation helped control the cancer, Dr Buckner said, ‘but at the cost of cognitive decline’….
Dr Paul Brown of the University of Texas MD Anderson Cancer in Houston led a study of 213 patients with one to three tumors in the brain to see whether the risks of whole brain radiation were worth its help in controlling cancer.
Half of the patients had the usual radiosurgery and the rest had that followed by whole brain radiation. Three months later, 92% of patients who got both treatments had cognitive decline versus 64% of those given just radiosurgery.
“The negative effects far outweigh any benefits” of the combination treatment, Brown said.
The other two studies involved when to remove lymph nodes, a place where cancer often spreads. Nodes help drain fluid throughout the body, and removing them leaves patients vulnerable to a host of complications, including painfully swollen limbs, infections and nerve damage.
Dr AK D’Cruz of Tata Memorial Hospital in Mumbai, India, led a study of 500 patients with oral cancer, usually tumors of the lips, tongue or mouth. …Nine months later, on average, researchers saw that removing the nodes cut the risk of death during the study by 36% and the risk of having cancer come back by 55%.
In the melanoma study, about 500 people in Germany with skin cancers on the legs, arms or trunk that had spread minimally to nearby lymph nodes were either given additional surgery to remove lymph nodes or just observed. Survival rates were comparable three years later, meaning the additional surgery was not worth the risk of its side effects.
Some doctors predicted the study would change care; others said they would wait to see if a second study underway now reaches the same conclusion. In any case, it’s worth a discussion between patients considering the operation, doctors said. [Emphasis added]
Here is the Independent article, by Caroline Mortimer 28 September, 2017:
NHS accused of ‘dereliction of duty’ for denying 43p-a-day drug to breast cancer sufferers
A number of cancer drugs entered the European market “without evidence of benefit on survival or quality of life”, researchers have said. All new cancer drugs are given Europe-wide market approval through the European Medicines Agency (EMA).
But a new study, published in The British Medical Journal (BMJ), found that of cancer drugs approved by the EMA between 2009 and 2013, 57% had no supporting evidence of better survival or quality of life when they entered the market.
After an average of five years of follow up, only half had shown a survival or quality of life gain over existing treatments or placebo. For the remaining 33 (49%), “uncertainty remains over whether the drugs extend survival or improve quality of life”, according to the authors from King’s College London and the London School of Economics and Political Science (LSE).
And of the 23 drugs with a survival benefit that could be scored with a validated tool, only 11 (48%) were judged to offer a clinically meaningful benefit, they added.
As a result of the findings, the researchers have called on the EMA to increase the evidence bar for the market authorisation of new cancer drugs.
Study author Huseyin Naci, assistant professor in LSE’s Department of Health Policy, said: “It is remarkable that so few cancer drugs enter the European market without any clear data on outcomes that matter to patients and their doctors: longer survival and better quality of life.”
I will end this GumshoeNews article by repeating the title of that Independent article. Namely: “NHS accused of ‘dereliction of duty’ for denying 43p-a-day drug to breast cancer sufferers”
(The NHS is Britain’s National Health Service.)At today’s exchange rate, “43p” is 76 cents Australian.
My point, however, is not that good medicine is withheld (that is the theme of my book) , but only that doctors do not appear to react when a treatment is found to be harmful.
Hmm.
–Mary W Maxwell welcomes comments below on layperson’s knowledge of cancer treatments.
You know I am in my usual blame-the-government, blame-the-doctors frame of mind, but I also blame the patients.
It seemed to me when I was in America recently that every family has an account at CVS (Consumer Value Store — a Pharma retailer with a few other things like cosmetics and greeting cards).
Why are people so trusting of all the doctors and hospitals? Geez.
I think it’s more a condition of powerlessness than trust and it sure is more common than not.
Everyone should have a check-list for dealing with the system, particularly in an emergency situation. No.1 would have to be “Be prepared to encounter hostility when you refuse a medication or procedure”. Also crucial to have in-person support on call.
I don’t do too badly, probably because I’ve had years of dealing with the so-called justice system. Which in my view is far more warped
“It is estimated that by 2020 more than half of all cancer in America will be medically induced from drugs or radiation, making our Medical establishment the leading cause of cancer. ”
– Dr. Ben Johnson, M.D., N.M.D, D.O.
with HRT prescriptions topping the list?
Quote, ” Why are people so trusting of all the doctors and hospitals?” Unquote. That’s easy to answer.
Because people have been conditioned via the MSM and even Movies and T.V. to believe that somehow Doctors are always right, and even weirdly, that Doctors never get it wrong.
Some Doctors even get sucked in to the hype and begin to believe they are some sort of higher life form and the rest of humanity should bow down at their knees.
Juts under two years ago, my wife fronted up for her regular mamogram, there was nothing untoward or suspicious, just the regular check up. Five weeks later, we get a phone call to front up at the Local Breast clinic for further evaluation, where we are informed a lump has been found on a breast and a lumpdecomy is called for to establish whether there is an cancer there. The operation was carried out there and then, no time given to consider and digest what we were told. The sample was sent off to the Lab and two hrs later we were told it was cancer type 2 and needed to be removed.
We were taken to another room wherein a Doctor took us thru the procedure involved, the removal of the offending lump,(No mention was made at that point, of Lymph Nodes being involved ) a aggressive course of Chem following the removal of said lump running for two weeks. Consisting of tuning up at the Chemo Center three times a week, sitting in a chair for three hours plus whilst the chem was pumped into the body. Then go home and suffer the side effects from the Chemo.
No one told us, the repercussions of the Chemo would result in hospital stays of two weeks fighting lung infections due to the destruction of the bodies ability to protect it’self.
Then the side effects of the chemo causing massive joint pains and diahrrea. Joint pains which still have not gone away to this very day.
The diahrrea was cause by the hormoun suppression medication, of whci there are only three options, all three were tried without success, so my wife flatly refused to take any more. Funny thing, the diahrrea disappeared. We later discovered mixing the Chemo and the Hormoun suppression medication was not a good idea, as once the Chemo ceased, and my wife again began the hormoun suppression medication, there was no side effect.
IMHO, the doctors should have been aware of this, and recognised it, yet the failed to do that.
Then there was the fluid build up in the body, we were told it was caused by the removal of the Lymph nodes, (19 in all ) of which only one was suspect. Until we complained of the fluid build up, NO ONE had advised us the Lymph nodes had been removed. We are then told the fluid build up was a consequence of the node removals and would be with us FOR LIFE. Next time you see a woman struggling to walk with grossly over sized legs and arms, she’s not FAT and LAZY, there’s a medical condition she’s got to put up with, that she was given no say in at all.
I could go on, fill up four or five pages easily or the arrogant behaviour of the medical profession against their patients especially when Cancer is involved.
But I have digressed from the question, ” Why are people so trusting of all the doctors and hospitals?” Where do you go, if you cant rely on your medical facilities when ill ????????????????
My God, Eddy, I don’t know how you’re still walkin’ the Earth after being treated so badly.
Unbelievable Eddy.
I listened to a lecture by Dr Ben Johnson. He was explaining how slowly breast cancer develops. from 1 cell to 2 cells 90 days, then it multiplies. It takes about 6-7 years for a lump to develop the size big enough for a mammogram. It is Dr J’s opinion that it is extremely negligent that anything is rushed.
I suggest you go to Truth About Cancer dot come. Some extraordinary info for what you need to do from hereon. I guess this is one of the most important resources for us at this time.
https://thetruthaboutcancer.com/
This is episode 1.
https://www.youtube.com/watch?v=gR8SQzCJK0Q
https://www.theguardian.com/politics/2002/apr/21/uk.medicalscience?CMP=share_btn_link
Thank you, Diane. That’s extremely helpful.
And then there is Maralinga–Ground zero
Think about this, people. Any other industry except the pharmaceutical market that puts a product for sale that then causes damage or injury to the user, if the product is used as advised, that producer can be charged with a crime, and must compensate the user. One law for all others but not for the industry that is allowed to make exorbitant profits with which to buy legislation, lawyers, judges and media.
“that producer can be charged with a crime,”
Mal, in US there is legislation to prevent lawsuits by the vaccine-damaged citizen, but surely there is no law against charging with crime any wrongdoer (such as the party that assaults you).
Commenters, please let me know if I am wrong on that. My belief is that in Oz, no one except the monarch is above the law (“the king can do no wrong”).
Consider this: we know that the FBI man who murdered Ibraghim Todashev in Florida “got away with it.” But this is because the public accepted the logic that it was up to the FBI boss to investigate and decide if that agent had done wrong. (Ridiculous).
The fault lies in us, IMHO. And only we citizens can overcome this state of affairs.
Medicine is currently hostage to a model known as “best practice”. In principle it sounds great, that the most proven treatments (backed by the god of peer reviewed research) are employed and older ideas are discarded as new and better research come along. I probably don’t need to point the obvious scope for corruptibility inherent in this as corporate contamination of research, and peer review occurs at every level. Why? If your product, procedure, device or whatever finds its way into the compendium of assumed “best practice” then the money rolls in, and we all know of the price-gouging that is modern medicine. Add to this a Deep State that doesn’t really want non-deep-staters living into an expensive old age, and you have a State/Corporate model of lifestyle management where one lives long enough to work, and is simply deleted in their later years, with their pocketbook cleaned out on the way to a premature grave, but all done in a sincere, caring manner. Perfect crime.
Ta, Paul.
All done with a smile for a room in a nursing home for $100 k per year .
Paul , thanks for a good conscise dose of the truth .
[…] was inspired to complete this article after reading what Eddy told us in GumshoeNews comment yesterday (February 21, […]
I thoroughly agree that MSM and FDA’s, TGA’s and university medical schools control the whole medical scene and people are blinded by them into believing what doctors advise. I stopped this belief nine years ago (2009) when all bloods came back showing no issues but I felt like I’d been run over by a bus. After an abundance of internet searches, trials including failures, I now take amazing supplements – herbs and minerals – that have transformed my well being completely. The main anti-cancer agents (preventative and curative) include IODINE/IODIDE, Ashwagandha, Cordyceps mushroom and HEAPS MORE. Way superior to mainstream medicine’s slash, poison and burn approach!!! Iodine builds up the body’s immunity while the other agents oxygenate the cells which stumps cell cancer growth. But there is an abundance of other herbs that also fight off free radicals and cancer cells.
PS. I loathe mainstream medicine’s term “standard of care”. To me it is a death sentence!